Comments
1. There is no scientific evidence that gender reassignment has a positive health effect.
Several studies show that it cannot be established that, in general and on the average, there is a positive health effect of gender reassignment treatments:
- In 2011, Dr. C. Dhejne, head of investigations (2020) of gender dysphoria in the department of ANOVA, Karolinska Hospital, Sweden, published a study (2011) that shows that for subjects who underwent sex-reassignment the risk of suicide is 19 times higher than the general population (x40 for girls who transition!). There is no indication or study that has shown that alternative or no treatment would lead to equal risk.
- Dr Stefan Arver, former head of the Gender identity service, ANOVA, Karolinska (2019), coauthored a report ordered by the Norwegian Directorate of Health, "Right to the right gender" (2015). The report states (page 3 line 3) that very little is known about the health effect of gender reassignment treatment.
- In an interview in "Världen idag" (Sweden), 2018, Arver states that gender reassignment does not reduce psychiatric problems of transpersons. This deserves attention due to the 75% to 87% co-morbidity of psychiatric diagnoses observed in the major, and new, young group suffering from gender dysphoria.
-
A "Health Technology Assessment" report from the Swedish public health care, "Region West", 2018, concluded the majority of studies on health effect outcomes of sex-reassignment-surgery are of low quality and lack evidence for a medical treatment protocol, a systematic review of 70 studies. The team included plastic surgeons who perform "gender-correcting" plastic surgery. They found that most subjects who had surgery perceived the changes as positive but the studies failed to show that SRS leads to an improved quality of life.
- Univ. Birmingham established a professional statistics centre, "ARIF". One task was to serve as advisors to the West Midlands Health Service to analyze novel medical treatments of disease. In a meta-study (100 studies) they concluded (2004, summary here under "Media -> Doc") that there is no statistically significant positive health effect from "gender correction" treatment. Furthermore, they write that many studies which present claims to the contrary are of a very low quality, with deficiencies in methodology and with an obvious "agenda" (political or ideological).
- The US GOV Department of Health in a systematic review concluded (2016) that most studies of health effets of SRS were of poor methodological quality and couldn't be used for evaluation of health benefits. The results of the few studies that passed the quality evaluation were too ambiguous to allow concluding that SRS gives a significant health benefit.
-
Chief Psychiatrist Dr. Paul McHugh, Johns Hopkins University Medical Center, USA, (one of the worlds most renowned medical centres and founder of child psychiatry as a medical practice) was active in the clinic that were the first in the US to refer transpersons to "sex reassignment surgery" (SRS). After 40 years of SRS, he writes (Wall St. J., 2017) that "We have made a mistake" (in performing SRS treatments) and acts to put a stop to SRS at the Johns Hopkins hospital (the largest hospital in the world).
-
The British Medical Journal published an editorial (2019) in which they concluded that gender-reassignment / affirmative treatment of children and adolescents must be considered experimental and is not evidence-based.
-
The UK Tavistock clinic is the only clinic in GB which offers investigation and treatment of children with gender dysphoria. Five employees recently resigned from this British National Health Service (NHS) clinic giving ethical grounds for their defection. They assert that the current treatment of children and adolescents is not based on medical science or experience. A Psychologist "whistle blower" at the GIDS unit claims confused children are wrongly being labelled transgender and referred to sex-reassignment surgery. (The US High Court in December 2020 ruled that minors can not give "Informed consent" and write that no evidence for medicalization treatment was presented).
-
An extensive study in Denmark (2016) which includes all individuals that underwent gender reassignment in Denmark concludes that mental health is not improved by gender reassignment, nor is suicide risk reduced.
-
GIDS, UK, report that suicide amongst children referred to the clinic is extremely rare (four in a decade of more than 7000 referrals, and those related to mental health issues). This should be judged in the light of the very high risk (19 times greater than general population, see above) of transitioned individuals.
- The independent Hayes inc. company researching clinical evidence for healthcare systems concluded that the evidence for medical treatment of gender dysphoria is "Very low certainty" (minirs) and "Low Certianty".
-
The Royal College of General Practitioners, the GP's association in the UK, recently published a report where they warn that the current treatment of children and adolescents with gender dysphoria in GB lacks medical scientific evidence. The Daily Mail presented a summary of the 12-page report. (7 July 2019).
- The Swedish National Board of Health and Welfare in collaboration with the Governments SBU authority in a systematic review (dec 2019) that there is no research evidence available demonstrating a benefit of "affirmative treatment" of children and in a new systematic review 2021 concluded that there is no evidence for medical treatments of minors; "Risk is greater than benefit", and concluded that medical treatment may be given only within the framework of an ethically approved research setting.
- The American Journal of Psychiatry (aug 2020) in an extraordinary correction of a publication from the Karolinska institute published a statement that the study failed to find evidence for a positive health effect of hormone treatment or sex reassignment surgery. This is, to date, the largest study of its kind with complete registered patient health data, not survey, not interviews, not self-report, and it failed to find any mental health benefit of hormones or gender affirming surgery.
- The Finnish Government comissioned a systematic review which in 2020 concluded that the evidence for medical treatment of gender dysohoria is poor (and recommends psycholigical ntervention as the first line of treatment for both minors and adults).
- The UK National Institute for Health and Care Excellence (NICE) in 2021 after systematic reviews concluded "Very low certainty" (there is no evidence) for medical treatment of minors suffering from gender dysphoria.
2. There are large unknowns on the number of regretters. (Long-term follow-up is lacking, but early "euphoria" that over time (average 10 years) turns into regret is well documented.)
The psychological barrier for a transperson, who transitioned with sex reassignment, to "come out" and admit he regrets, is enormous. Even so called desisters who only went through a social transition report that they considered committing suicide rather than facing friends and society after admitting that they realized they had been confused, they got it wrong, that they are in fact content with their biological sex/gender.
The Karolinska Hospital, Sweden, states in media (both in Norway and in Sweden) that they find very few individuals who regret, about 2%, in their studies. This number lacks proper critical analysis and anchoring. Typically, claims "Only 2% say they regret" are vague and imprecise. is an attempt to evade rigorous investigation and objective analysis. Conclusions cannot be based on what the clinic means patients "say". In their reports. However, it is clear that even this is an overstatement, they only counted as an instance of "regret" if a patient requested a medical detransition. Those who committed suicide or did not agree to participate or who cannot be located, or who only "said" they regret were not counted in this study.
Thus, Karolinska's figures relate only to the small group of patients who formally asked for a medical "detransition". This arbitrary and obviously false definition of who are "regretters" is unacceptable. It is known that the majority of individuals who regret blame themselves for their erroneous "gender correction". They don't, generally, blame the health care sector, the psychiatrists and investigators. They are ashamed or do not dare take the step to ask for a detransition.They also experience pressure from and loyalty conflicts with previous friends in the trans-activist environment.
Most studies who try to estimate "regretters" report that generally regretters don't want to cooperate and there are large "fallouts", missing subjects in the analyses, of the order of 50% (e.g. 36%, Wiepjes et al. 2018).
Comparable figures from the US and GB show around 10% who regret of this same category of transpersons as defined by the Karolinska, i.e the small subclass of those who regret and formally contact the health care sector to request a detransition
Recent numbers on official detransitioners indicate higher frequencies of detransition. If one assumes equal percentages of friends, close of kin and supporters both in "transgender" and in "detransitioners" groups, then the number of offical detransitioners would be of the order of 15% (i.e. also not including the "hidden" regretters).
Furthermore, the Karolinska Hospital investigators have systematically avoided rigorous follow up of patients and sent out questionnaires typically less than 6 months after surgery, with questions about whether they are satisfied with the gender reassignment. Long-term follow-ups are missing (even though these are required by Swedish legislation). The typical time to regret after transition, however, is about 10 years (Wiepjes et al. 2018). That the Karolinska doctors don't mention the problems that lie in their inadequate definition, in the lack of follow-up renders the Karolinska's objectivity questionable.
3. Co-occurence of psychiatric problems is very high, major studies conclude 75 - 88%.
Many studies show that there is a very high degree of comorbidity (gender dysphoria is also healt h issue requiring treatment) with psychiatric problems among those with gender dysphoria. (Activists for transgender people's right to gender reassignment treatments oppose the term co-morbidity, but this is only a semantic issue that is not medically relevant here and also not to the WHO ICD-11 coding of illness). More recent studies from Finland , the US and Australia, conclude that the co-morbidity with significant psychiatric issues is 75 - 88%. Previous studies from non-Scandinavian countries also show very high numbers. A new development is that previously were psychiatric issues higher for men/ boys (transwomen).The study from Finland shows that the co-morbidity of mental issues for women/ girls (transmen) has "caught up" with those for transwomen (boys at birth).
The Australian study investigated attachment problems as a common cause of childhood development of gender dysphoria and found 88% psychiatric diagnosis comorbidity Since the attachment problems develop early this study also contradicts the hypothesis that mental health issues are the result of social stigma.
The ANOVA clinic, the Karolinska Hospital, Sweden, presents a low incidence (about 4%) of mental health comorbidity (C Dhejne et al., 2016) in their summary, claiming also it improves with surgery but evidence was not presented. The data are from a "meta study", i.e, not the clinic's own comprehensive database of registered data, and neglects presenting the limitations in their summary. This summary lacks credibility since it so distinctly differs from other studies and international consensus.
It is remarkable that the summary in the publication fails to mention that autism spectrum disorders (ASD) in those with gender dysphoria was also not included in the compilation. It is startling for a summary which authorities and interest groups will read and which characterizes mental illness, as it is well known that ASD is the most dominant psychiatric issue correlating with gender dysphoria. The British NHS reports about 35% comorbidity, a major Finnish study indicates an order of 25%. This psychiatric co-occurrence is well known since the early 1990s, with hundreds of published reports. It is noteworthy that Karolinska's summary does not mention this important limitation in an article dealing with the frequency of psychiatric illness seen in the transgender ppopulation.
Equally noteworthy is their claim that mental health problems decrease after gender correction, sex-reassignment. This is in contradiction with international consensus and (see above under 1) statements by the former head of the ANOVA clinic.
Mental problems in girls have increased dramatically over the past ten years. At the same time, gender dysphoria of that group has increased. Research attempts to clarify the causal link for these rapid negative developments are yet to be presented.
In recent years psychiatric problems of young girls have increased dramatically in parallell with an increase in gender dysphoria. GD for boys has has also had an avalanche-like increase but the GD for boys lags a few years, in their debuted age, behind that of the girls. Research is yet to unravel the cause of these developments.
In Sweden the Karolinska hospital (KS) stipulate that the exceptional increase is a result of the change in Swedish legislation in 2013, when it became possible to change official gender without the demand of sterilization. This explanation is not compatible with the observations that
a) the same development is seen in all Western countries, Europe and the USA.
b) There is a correlated dramatic increase also in psychiatric related problems in the same age group (anxiety, self-harm, anorexia, depression)
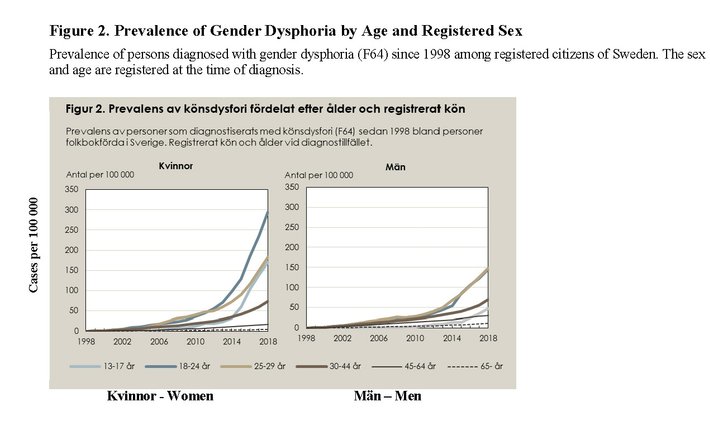
c) There are large differences in debut age of the development of GD for boys and girls that remain the same after 2013 (Marchiano, 2017 Fig.1 and figure above). Had the KS hypothesis been valid then changes in 2013 should have been parallel for boys and girls and also seen with adults who wish to transition.
It is worrying that KS don't discuss the problems with a hypothesis which hinders evaluation of the roles of social contagion, elements , the well known "body focus" and pressures on young girls and the influence of social network availability.
4. Gender reassignment (hormones and or surgery) does not reduce psychiatric problems.
As noted (1. above), the largest objective study to date (sept 2020) of the effects of sex-reassignment-surgery (SRS) on mental health, failed to show any mental health benefit from hormones or "gender affirming" treatment. The study is objective because it is based on registered patients in Sweden who received "gender affirming" treatment as well as on their health records also many years after hormone treatment or surgery.
The authors first reported such a benefit, but the study was corrected by the journal, American Journal of Psychiatry, by both Universities who hosted the research (Yale Univ. and the Karolinska Institute) after severe criticism from seven letters to the editor. Unfortunately all the "retractions" and letters to the editor and the chief editor's retraction are behind the "paywall" and the misleading title of the original paper was not changed. A full account, including the authors' own evidence (in their retraction) that there is in fact no benefit from SRS can be found here (In particular, see the graph).
"Medscape", administering the Continued Medical Education (CME) for MD’s., in November 2020 withdrew their mention of the Karolinska conclusions and notified 6400 MD’s of the erroneous information for treatment of Gender Dysphoria.
Norwegian media has repeatedly reported (Aftenposten 2018, "At Torp" (Benestad), NRK, 2019) that mental problems disappear after gender reassignment treatment. These completely erroneous claims are spread by so-called activists in Norway with an ideological agenda that they give priority over the medical research conclusions. They wish to take over treatment from the Hospital (NBTK, Norway) also of children and adolescents. There is now an international consensus of that the claims are false, i.e. the psychological problems do not disappear, they don't even diminish, after sex reassignment treatment.
5. Suicide risk does not decrease after gender reassignment treatment.
Misleading information is regularly provided by activists that providing gender reassignment treatment, hormones, puberty blockers is justified due to the risk that people who suffer from gender dysphoria will commit suicide if they do not receive "gender affirming" health care (i.e. involving adaptation to the self identified sex). The arguments are false, since repeated studies [ a, b, c ] have established that suicide risk does not diminish with gender reassignment. See section (1) above. Claims that studies show otherwise are based on surveys with methodological errors (see section 1, US GOV. CMS review, and SEGM.ORG info site).
A detailed analysis of studies of suicidality of transgender persons reveals many caveats, se review by Zucker, many with selection bias.
In the non-representative US Transgender survey 2015 one conclusion was that lifetime risk of transpersons suicide attempt is 40%. (It may be noted that this survey was done by "transactivists", positive to gender affirming care). This is likely a too high "estimate" by the survey but it contrasts with reports from the GIDS unit for referral of all children and youth in the UK, that suicide during investigation (i.e. prior to transitioning) is "extremely rare". In the past decade there have been four suicides amongst more than 7000 referred to the clinic, and these were related to psychiatric issues. These numbers indicate that suicide risk after transitioning increases; there is no study to show that it that it decreases. This conclusion is also consistent with the x19 higher risk for suicide (than general population) found by Dhejne et al. (see top of section 1). They can not present equivalent data for alternative treatments to GD issues.
The Swedish National Board of Health and Welfare presented data (Unofficial English transation) indicating that the risk for suicide for all major psychiatric illnesses are significantly larger than that of suicide risk due to gender dysphoria, indicating that the major risk for suicide for GD patients is due to the high comorbidity of mental health issues.
6. One must begin by investigating psychiatric issues. Affirmative treatment must not start before evaluation.
7. Only teams of experts with long clinical experience in making psychiatric diagnoses should investigate children/ adolescents.
The Endocrinological Society has written "International Guidelines" for the investigation and care of gender incongruence / transsexualism / gender dysphoria. The guideline emphasizes that all treatment of children and adolescents must be preceded by extensive psychiatric investigation by professional clinicians. These are their starting sections, 1.1 and 1.2, in the "International Guidelines". The Endocrinological Society specifies that only psychiatrists with (long) experience of giving clinical psychiatric diagnoses should perform the psychiatric evaluation of children and adolescents and that investigations should be done by a team of experts.
Consistent with these directives is the warning by the well known group in Amsterdam that also an affirmative treatment involving only "social transitioning" is deprecated since it may consolidate gender dysphoria.
"The World Professional Association for Transgender Health (WPATH)" guidelines, the so called "Standards of Care" (SOC-7), is a similar guideline but with a number of critical differences. In comparison with the Endocr Soc guidelines, SOC-7 was not approved exclusively by professionals, but by individuals who do not necessarily have the support of research groups, experienced healthcare providers or clinical investigators. SOC-7 also does not differentiate between the required basic qualifications in psychiatric competence for the investigation of children/ adolescents and the basic qualifications required for the investigation of adults. The Endocr Soc guidelines maintain higher standards with specific requirements for investigators of children and adolescents.
The Endocr Soc guidelines also explicitly notes that the guidelines are not evidence based.
In contrast, SOC-7 does not clarify that SOC-7 is not evidence based. SOC-7 is also not recognized as a medical guideline by the medical evidence based guideline database at ECRI.
SOC-7 presents examples of basic qualifications for psychiatric competence for investigation, e.g. "a couple's counsellor" or a nurse. There is no specification of specialty medical psychiatric expertise, University level education in psychology, or experience. Thus, according to SOC-7, a couple's therapist or a nurse who has passed the basic nurse education exam has the required basic qualifications to do psychiatric investigation also of children and adolescents. There are no directives in SOC-7 or objective requirements on psychiatric competence for the investigator's competence.
"The American Association of Pediatrics (AAP)" has also written guidelines for the care of gender dysphoria. These are written by, in principle, a single person.
Finland in 2020 presented new guidelines for young, adults and "non-binary". For all categories psychiatric care and investigation is instructed as the first line of treatment.
In 2022 Sweden published new recommendation guidelines emphasizing psychiatric evaluation in the primary phase of evalaution and treatment.
8. Children/ adolescents grow out of the gender incongruence (80 - 90%) while on the other hand ...
Many studies show that children grow out of sex incongruence during puberty. "Activists" have tried to reject these studies, but the criticisms are very superficial. Arguments address problems in uncertainties in which children / adolescents are to be regarded as being transgender, e.g. some will turn out to be homosexual but not have identity problems. Such ambiguities are always present in the investigation before puberty, but even with very restrictive interpretations the proportion that grow out of gender dysphoria is very high, if not 90% then 70%.
Dysphoria was previously diagnosed with the psychiatric "manual" DSM-III but with DSM-V, as well as current reliance of "self-diagnoses", the very inclusive protocols of, e.g., The Karolinska and the increasing trend of both parents and children themselves to interpret their behaviour as transgender and dysphoric then the higher number is likely more correct.
One argument put forward is that only children who, after puberty, still show gender dysphoria should have been counted in the group of children who were "truly" gender dysphoric, i.e. that the others included in the group were mistakenly included. Such a "retrospective" adjustment of who should be considered to have suffered from gender incongruence/ dysphoria invalidates a major aim of the study, to evaluate the prognostic value of diagnosis. Arguments that gender incongruence or same sex sexual preference was confounded with gender dysphoria are irrelevant since it is impossible to predict if a gender incongruent behaviour of, e.g., a nine-year old will persist as gender dysphoria during puberty. There is no reliable examination to differentiate between gender dysphoria and gender incongruent behaviour in a child who believes he/ she is "born in the wrong body" (or wishes to be "the other gender"). Similarly, it is increasingly difficult to predict if gender incongruent behaviour will manifest as gender dysphoria during puberty, in part because of escalating contagion from social media incitements. Thus, there is a huge risk that puberty blockers are given in error.
Irrelevant arguments have been put forward to claim that only those who, after puberty has already begun, still show gender dysphoria should have been included in the study. This is just another twist of the above false argument. Statistically, it is clear that the small group (10-20%) who in the end will have lasting gender dysphoria, will obviously take up a greater and greater part of the "non-desisters" as puberty proceeds. Their proportion will be falsely increased the longer puberty progresses, after more and more children have desisted, leaving ony the ones that did not. It is irrelevant with such an analysis to evaluate how many people become desisters. The interest of medical practice is in the uncertainty of the initial psychiatric evaluation. The important point remains, up to 90% of all prepubertals with the gender incongruence will grow out of it.
9. .... treatment with puberty blockers consolidates gender dysphoria in 100% of treated children/ adolescents
It is grave that many care givers who act for the rights of transpersons do not admit or fully consider the risk of making an error, which is huge, if one starts treating children before puberty with puberty blockers. Recent research shows that "affirmative" treatment leads to irreversible fortification of the gender dysphoria.
In Sweden and Norway, so called "trans activists" are actively pursuing the unchallenged affirmative treatment of transpersons. This is also the situation at the Karolinska Hospital's Department for Children gender dysphoria investigation (KID), also at the children and adolescent Psychiatric clinic, a number of private clinics with uncertain expertise, psychiatrists and psychologists. The risk that affirmative treatment "consolidates" the child gender dysphoria is enormous, since the risk (see section 8) is between 8: 1 and 9: 1 that the child would have become a desister without affirmative interference.
The procedure followed by those who support affirmative treatment of gender dysphoria in children is contrary to the findings in all recent research and is not evidence-based. There is no psychiatric or other medical evidence that supports these treatment protocols.
10. Treatment with puberty blockers increases mental health problems in girls. Gender dysphoria does not decrease.
11. There are serious medical risks and side effects of puberty blockers and hormone treatment.
More and more reports are coming that not only hormone treatment but also puberty blockers are not reversible and harmless, but on the contrary are strongly associated with medical and mental health risks. The myths that puberty blockers are harmless are old hypotheses before studies and follow-up investigations were published. Risk of irreversible infertility as well as irreversible effects on bone density (e.g. chronic spine issues, effects on ribs,) and lowered IQ (up to about 8 points, due to arrest of brain development) were noted.
In addition to these studies (see REFERENCES), the British NHS has recently made follow-up studies of the effects of puberty blockers on children and analysis of these data show that psychiatric problems (suicidal thoughts, self-harm, anxiety, gender incongruence - i.e. dissatisfaction with some gender aspects of their body characteristics) increased in girls after treatment with puberty blockers.
Oestrogen treatment of transwomen increases the risk of ischemic stroke by 250%. Testosterone treatment of transmen can give extreme acne problems. Are these medical issues properly discussed with patients?
Regardless of the medical findings in recent research, the treatment with puberty blockers is unethical since (see section 9 above) puberty blockers consolidates gender dysphoria in children who would otherwise "grow out" of it. One risks destroying the lives of children who would otherwise grow into a "normal" adult role.
12. It is a myth that specific brain regions of trans persons are more like those of the self-identified gender.
A false argument put forward (also in an interview with the chief investigator at ANOVA, Karolinska Hospital, Sweden, in the program "The transtrain and the teenage girls"), is that certain brain structures in transgender persons have characteristics that are more similar to the "perceived" gender than the "assigned" gender.
A similarly unjustified claim was advanced by six MD's at the Karolinska institute in the Swedish Medical Society Journal, that transsexualism is established already early in development (i.e implicating "in the foetus") . No evidence for this was presented and it is contradicted by all clinical science and experience. The vast majority of referrals today are from teenage girls with no childhood history of gender incongruence.
All such similar claims of structure similarity are myths and refuted by technically advanced methods in morphological studies of brains of transgender and control groups.
There are differences between men's and women's brains, statistically. For example, male brains are on the average 10% larger than female brains. Women have a higher density of "gray matter" (abundance of neuronal cell nuclei) and, correspondingly, the volume of "white matter" (abundance of non-neuronal glia cells, in particular "myelination" of neurons) in men is larger. The cerebral cortex of men is thinner than that of women. (It should be noted that the proportion of non-neuronal, astrocyte glia cells to nerve cells is much higher in human than in other animal species, only elephants and dolphins have similar high amounts of glial cells and there is no simple relationship between the number of nerve cells, glial cells, myelinated nerve cells and brain function).
Extensive studies of human brains have been made with so-called Functional Magnetic Resonance Imaging (fMRI). The conclusions were that the variability in each region, "nucleus", is so large that it is impossible to say this region shows that this brain belongs to male or a female. Nevertheless, "deep learning" computer programs can "see" with 93% accuracy (so far) that there are two classes of brains, male and female.
In transwomen (born male) brain morphology differences to a control group of men were found, but the differences observed were identical to those seen for homosexual men and were not more similar to female brain morphology. A similar relationship was seen between transmen (biological female), lesbians and a control group of women. Thus, the brain morphologies that can be determined with scanning imaging indicate sexuality and nt gender identity.
Similar studies have been made of changes in brain structures for different professional occupations. For example, a long-term study of comparison between stewardesses (airplane) and taxi drivers (in London) showed that the profession over time can have a major impact on the size of brain structures, such as the hippocampus a brain structure known to be critical to memory and spatial orientation processing. Also, studies of various mental disorders (e.g. schizophrenia, depression, sleep deprivation) also show significant differences to control groups.
Differences of brain morphology of individuals suffering from gender dysphoria, when compared with control groups, are also likley conflated by diferences seen for various psychiatric disorders and psychosocial stress, greater for transwomen (born males) than for transmen. It is well known that transwomen have more difficulty in adjusting to the transgender role and of being "passed"/accepted by society, compared to transmen. Transwomen experience a greater mental strain in their changed role. In summary, there is no evidence that the transwoman brain is more like the control group women's brains, nor are there any corresponding differences in the transmen brains. Both claims are false citations of science data.
In children, the brain is not fully developed and is programmed to change with age, genetically and when exposed to sex-specific hormones. During puberty testosterone in males leads to the cerebral cortex being thinned in relation to that of females and then becomes "male" in its characteristics.
As a consequence it may also be noted that, thus, one cannot know, before puberty, details of how the brain will develop during and after puberty (up to the age of 25). It is therefore impossible, even theoretically, to use fMRI in children to try to draw conclusions about whether the child suffers from gender dysphoria or suffers from other psychological/ psychosocial issues.
GENID Norge
Gender Identity Challenge - Norway
Org.nr 924 796 359
Bankgiro:
1506 42 41009
Vipps:
606367
Kontakt
Epost: post@genderchallenge.no
De fleste av oss er anonyme i offentligheten av respekt for barnas privatliv. Men send oss gjerne en e-post hvis du ønsker å komme i kontakt med oss.
Er du pårørende til et barn eller ungdom med kjønnsdysfori, er du velkommen til å bli medlem i Genid.
Medlemskap er også åpent for profesjonsutøvere og forskere som ønsker å engasjere seg i Genid. Ta kontakt med oss på epost hvis du ønsker å bli medlem.